This model attempts to predict morbidity and mortality outcome from admission physiologic data for patients with suspected brain injury. Derived from the TOPICC study, the target population is for all pediatric patients admitted to the Pediatric ICU where the clinician has suspicion of brain injury on admission, regardless of primary diagnosis. It does not apply to neonatal ICU patients. Input includes basic demographics like age and sex, and all physiologic parameters required to perform a PRISM score from 2 hours prior to admission to 4 hours after admission. Output includes three potential outcomes: death, survival with a new reduction in functional status (morbidity), and survival with unchanged functional status. The functional status was calculated by the difference in Functional Status Scale (FSS) score at hospital discharge.
This model is only applicable to:
Excluded:
Publication entitled "Interoperable and Explainable Machine Learning Modeling to Predict Morbidity and Mortality in Pediatric Patients with Acute Neurological Injury in the Pediatric Intensive Care Unit" is in submission.
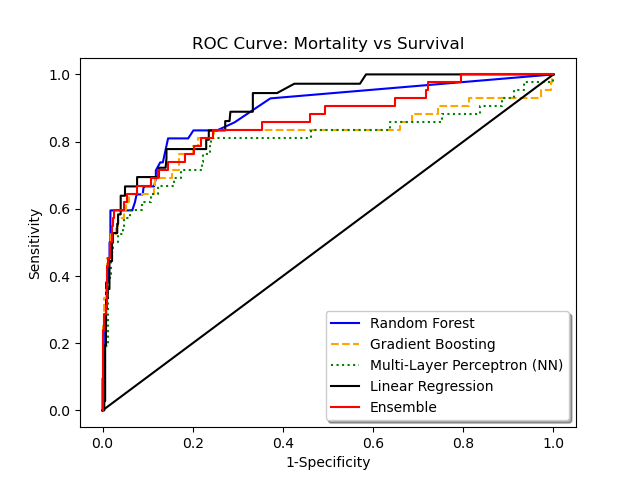
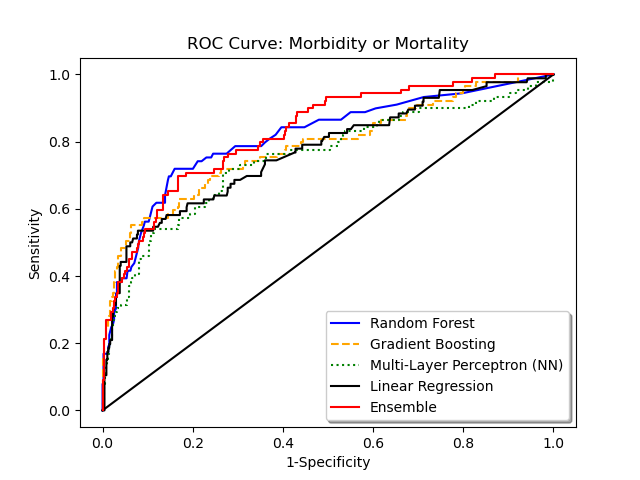
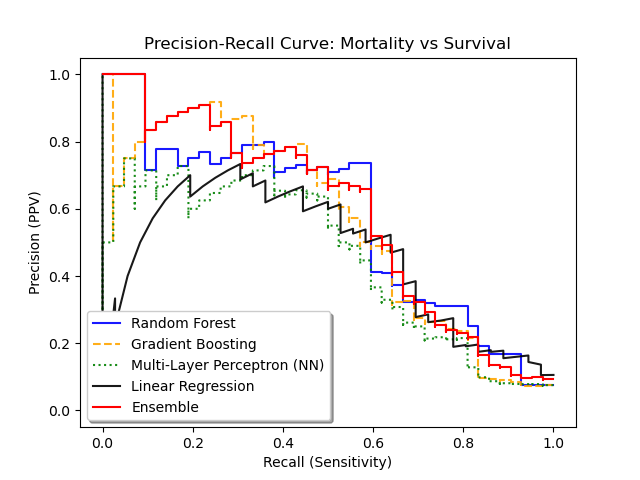
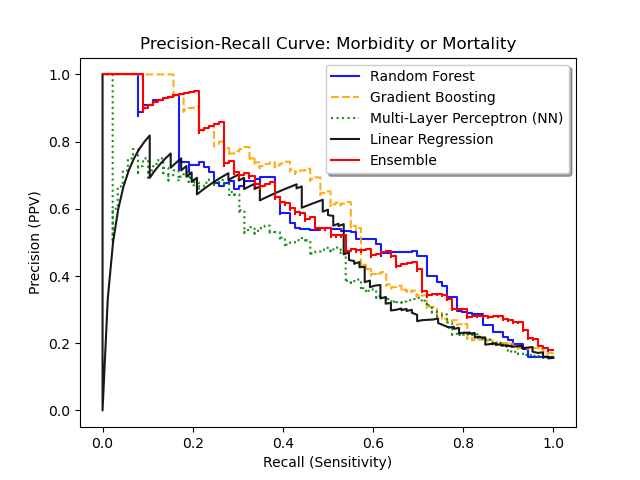
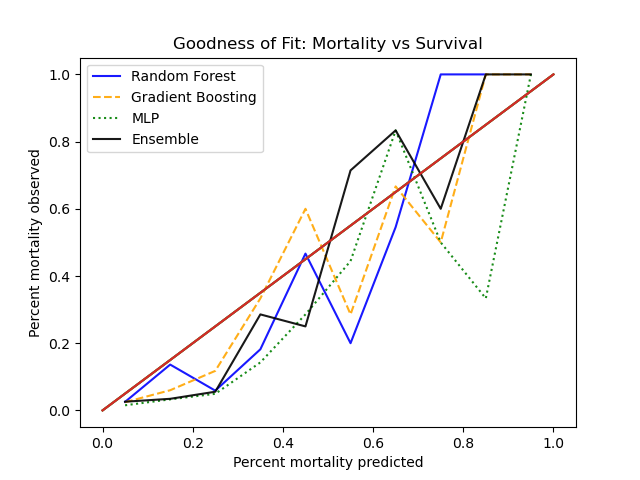
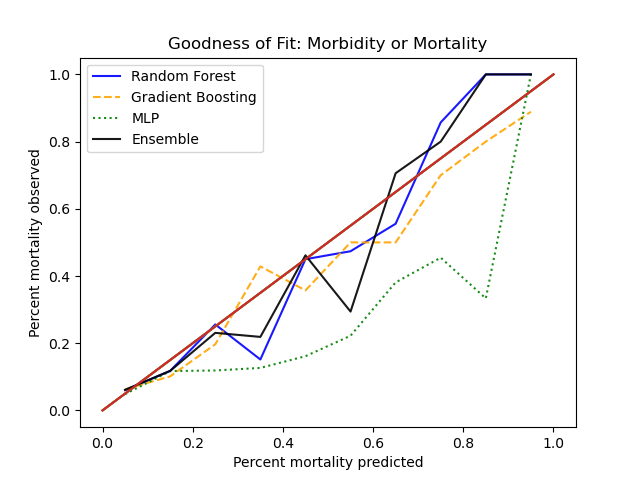
In the original cohort, mortality was 6.2% and morbidity 8.2%. The random forest model performance is as follows:
Graphical representation of the ROC and precision-recall curves is given below, in comparison to other algorithms. Calibration curves using Hosmer-Lemeshow goodness-of-fit is given as well.
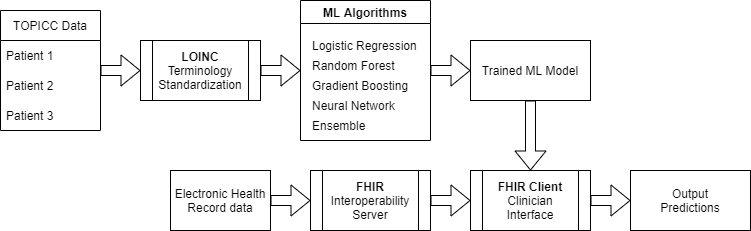
This proof-of-concept application demonstrates real-world usage of a predictive model using FHIR (Fast Healthcare Interoperability Resources). The FHIR server contains generated/synthetic data for sample patients and includes demographics, vital signs, and laboratory values using interoperable LOINC coding, as would be done in a real FHIR deployment. The application polls this simulated Electronic Health Record database in real-time to extract values needed for the model (physiologic parameters from the first 4 hours of admission). The pre-trained Random Forest models for mortality and morbidity/mortality are run, and the explanatory model demonstrates which features in this patient's physiology are most predictive of outcome.
Author: Neil Munjal, MD. Neil is a dual-trained pediatric intensivist and child neurologist in the department of Critical Care Medicine at the University of Pittsburgh and UPMC Children's Hospital of Pittsburgh. He is also a Machine Learning and informatics-focused computer scientist with particular interests in real-time neuro-ICU monitoring and causal inference methods using EHR data. He can be reached at firstname.lastname @ chp . edu.